V. Dimov, M.D., Clinical Assistant Professor of Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, Ohio; B. Altaqi, M.D., Assistant Clinical Professor of Medicine, University of Louisville, Kentucky
See the slide show or click on the images below for step-by-step instructions. A free PDA version of this procedure guide is available from MeisterMed, iSilo reader for PDA is required to view the images.
Indications
Pleural effusion which needs diagnostic work-up
Symptomatic treatment of a large pleural effusion
Contraindications
Uncooperative patient
Uncorrected bleeding diathesis
Chest wall cellulitis at the site of puncture
Relative contraindications
Bullous disease, e.g. emphysema
Positive end-expiratory pressure (PEEP) mechanical ventilation
Only one functioning lung
Small volume of fluid (less than 1 cm thickness on a lateral decubitus film)
Procedure Step-by-Step
Explain the procedure to the patient and obtain a written informed consent, if possible. Explain the risks, benefits and alternatives (RBA). Benefits may include less SOB, obtaining a diagnosis, and risks may include pneumothorax, bleeding, or even death.
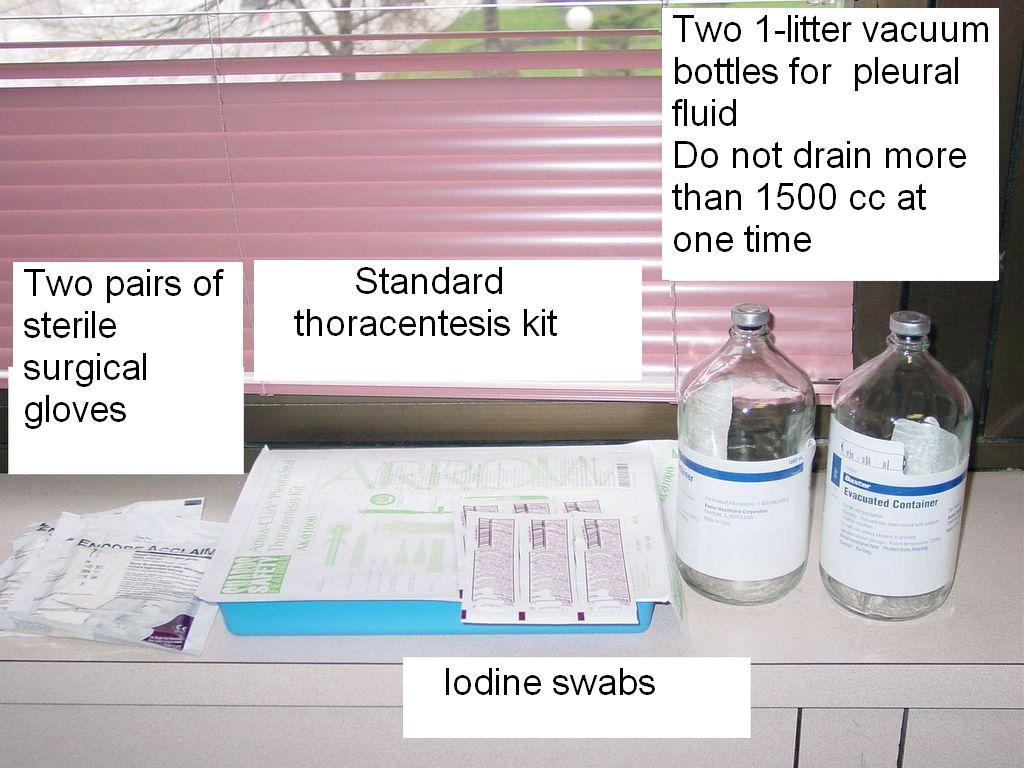
Fig. 1. Get the standard thoracentesis kit. In addition to the kit, you will need two 1-liter vacuum bottles and Bethadine for cleaning the area. Prepare the necessary equipment for the pleural tap.

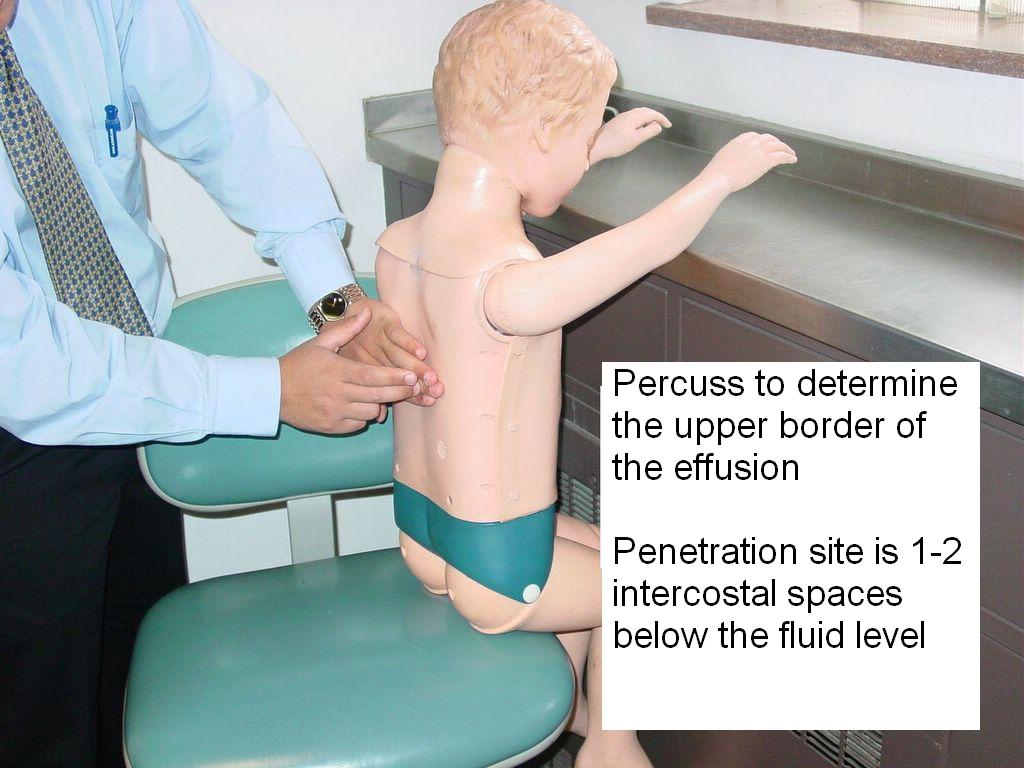

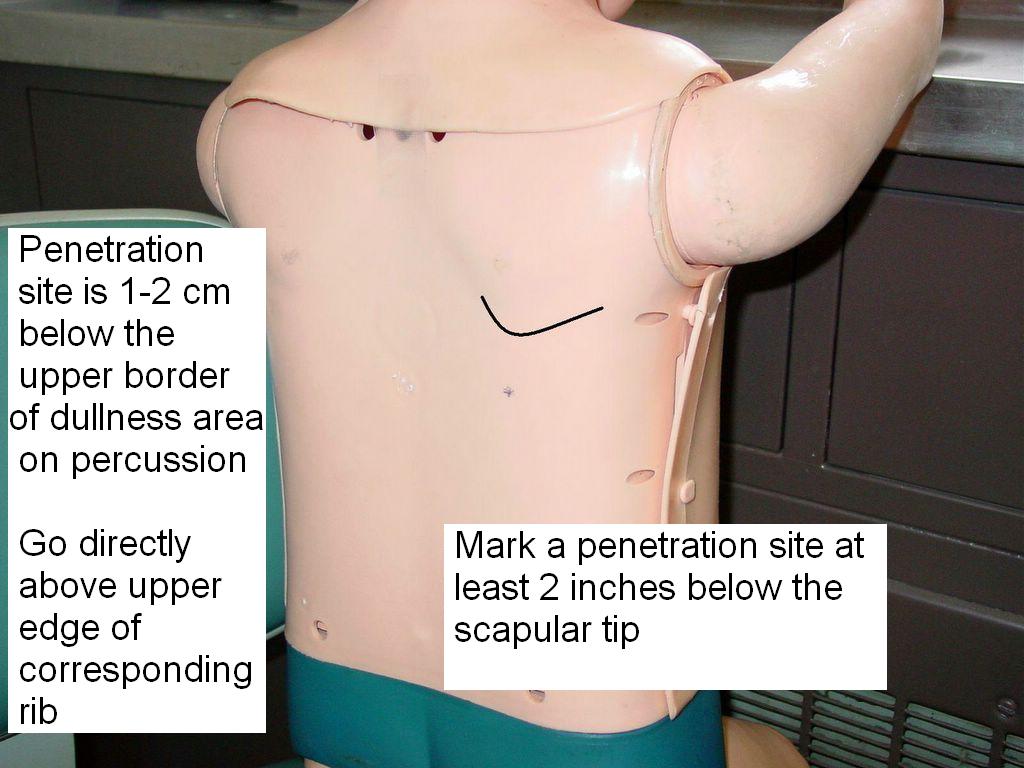
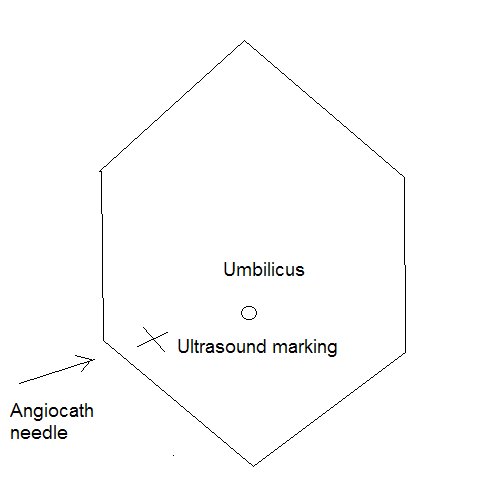
Fig. 2, 3, 4, 5. Find the anatomical landmarks before you perform the thoracentesis.


Fig. 6, 7. Clean the area with iodine.
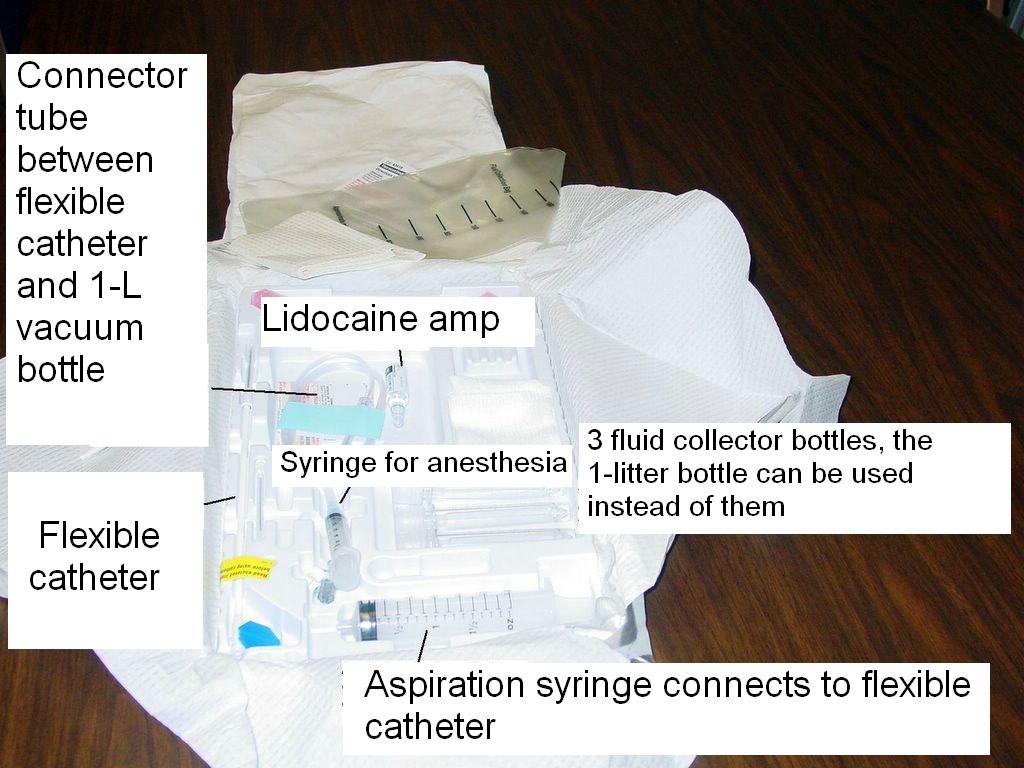

Fig. 8, 9. Open the kit and make sure that you know which tube and needle are used for.

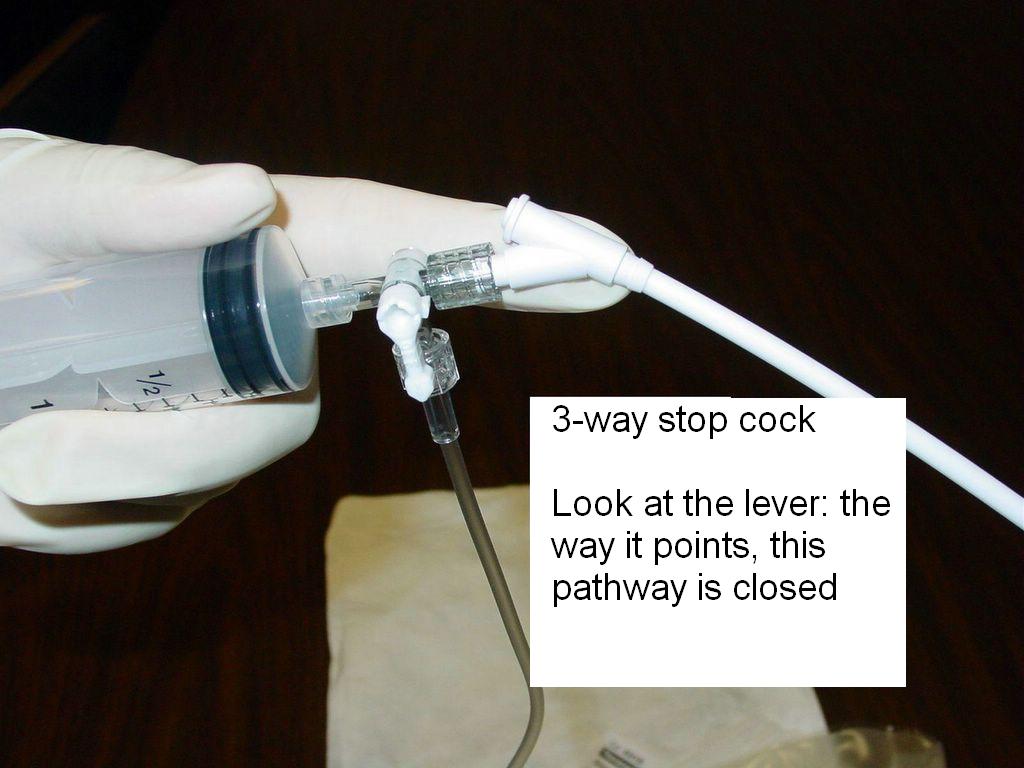
Fig. 10, 11. Practice sliding the flexible catheter.


Fig. 12, 13. Prepare for local anesthesia.


Fig. 14, 15. Prepare the area.
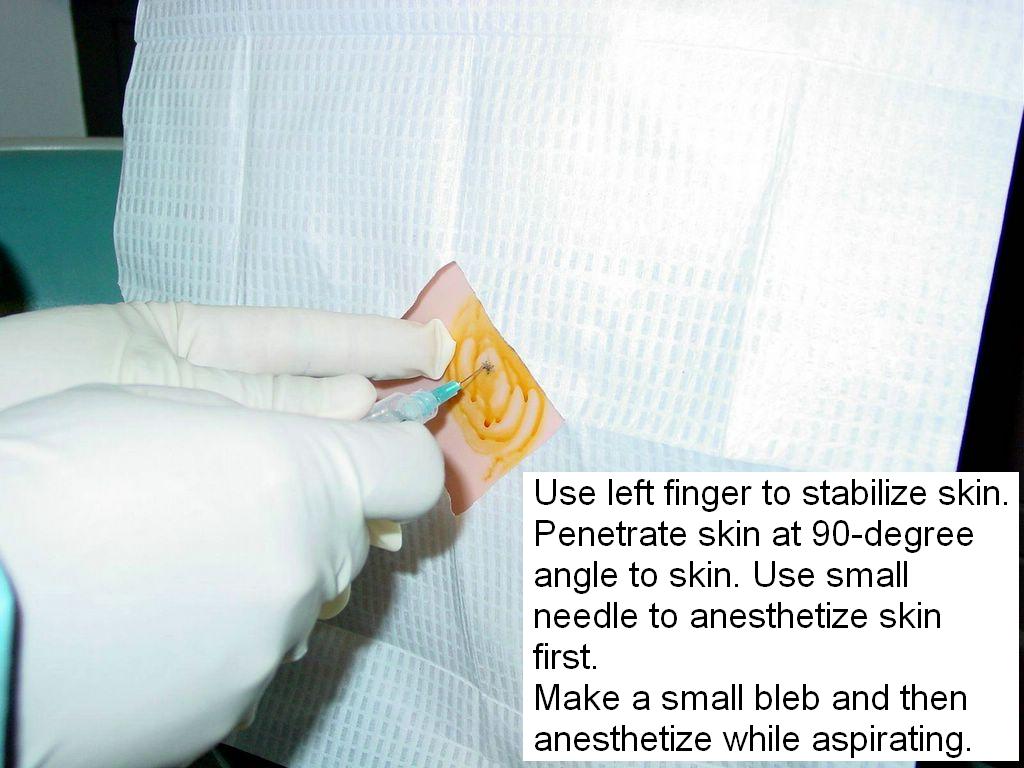

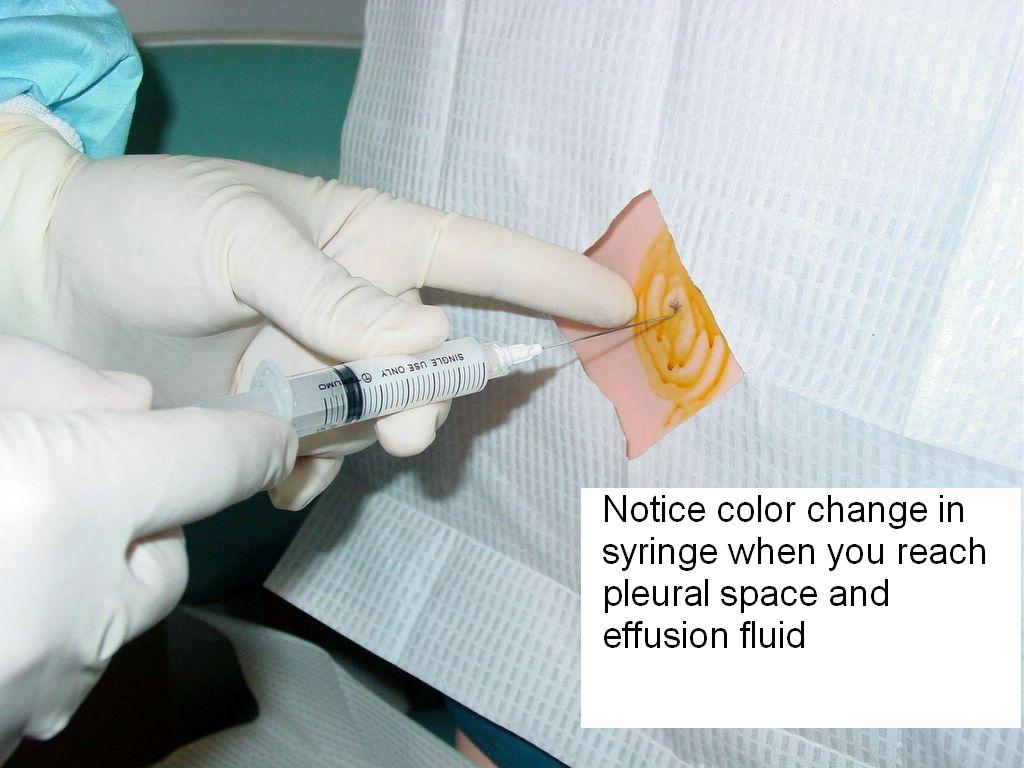
Fig. 16, 17, 18. Perform the procedure (under supervision, if you are not certified). Anesthetize the skin and pleura, try to reach the effusion fluid.
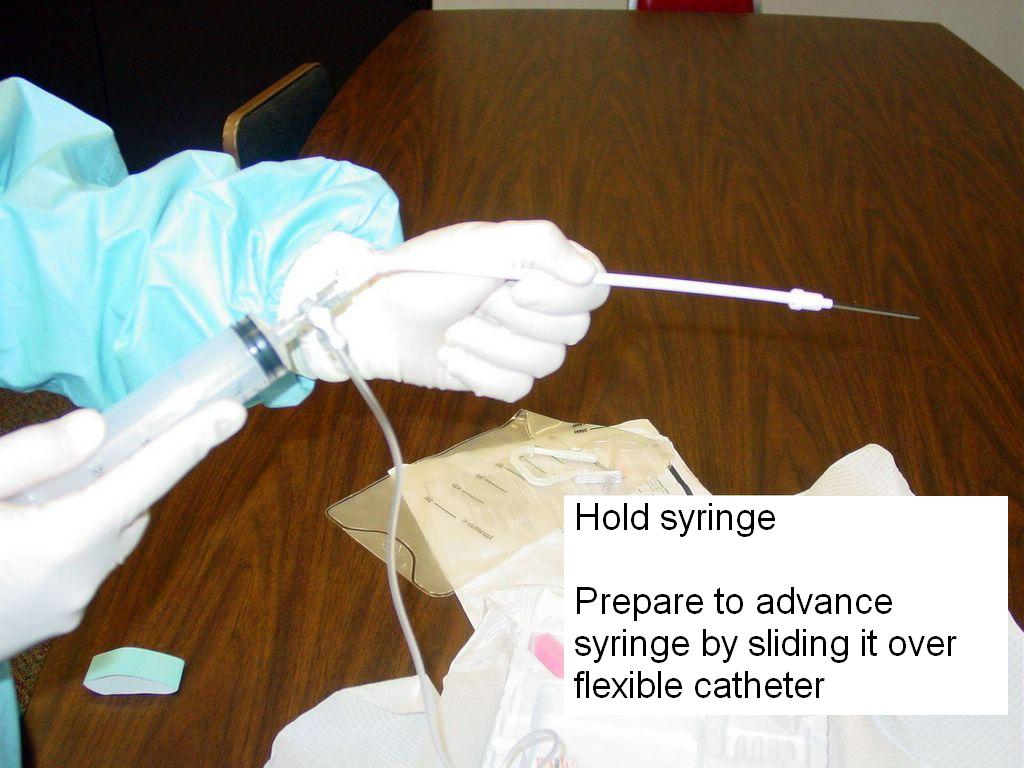
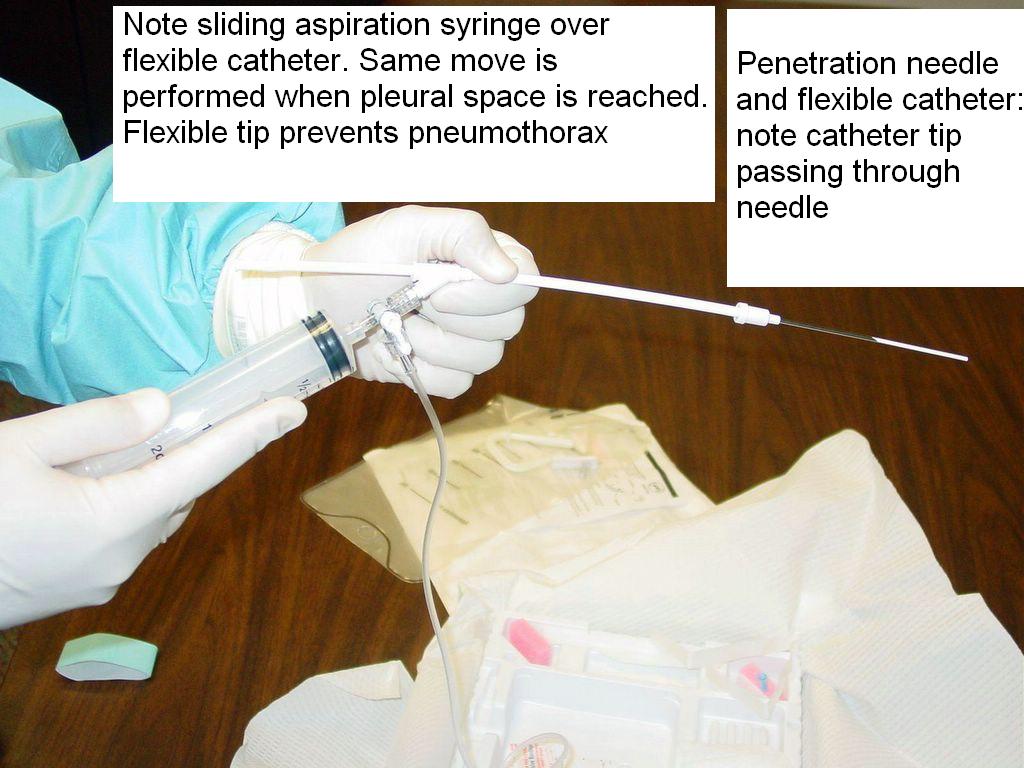
Fig. 19, 20. Prepare the flexible catheter.
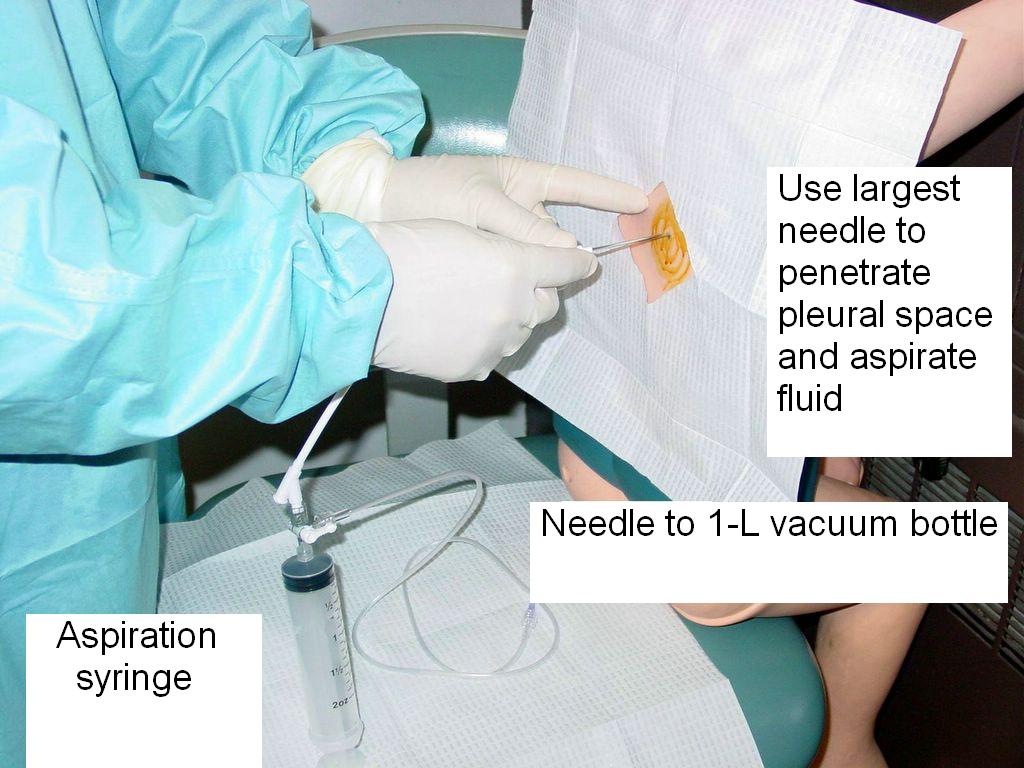

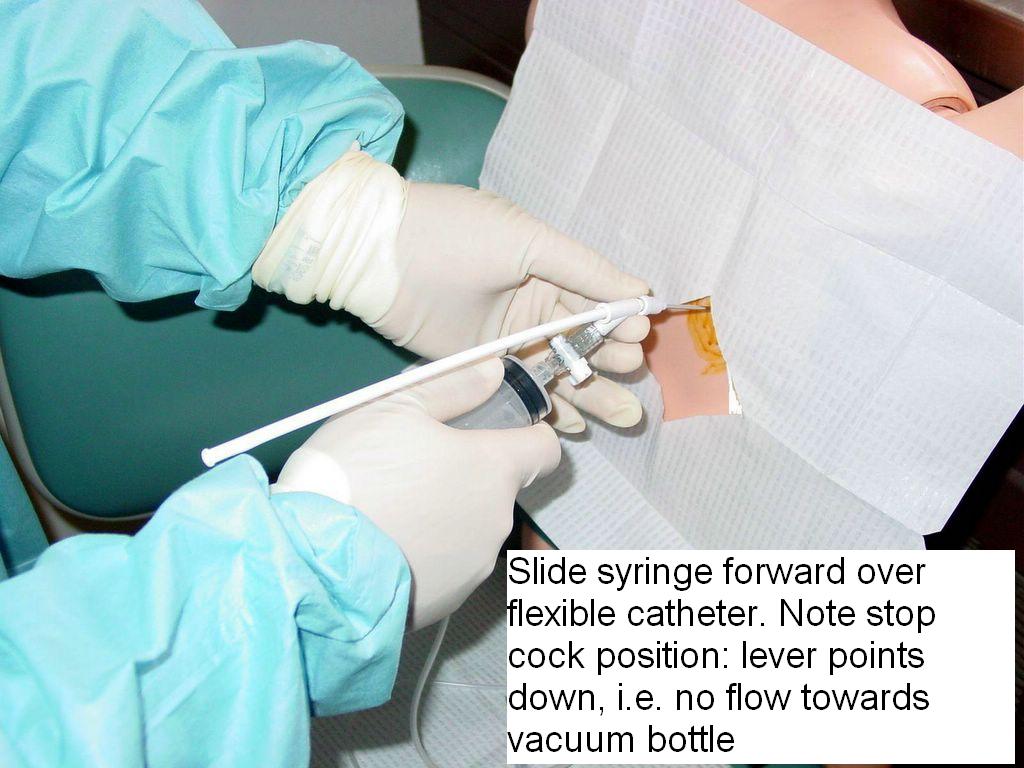

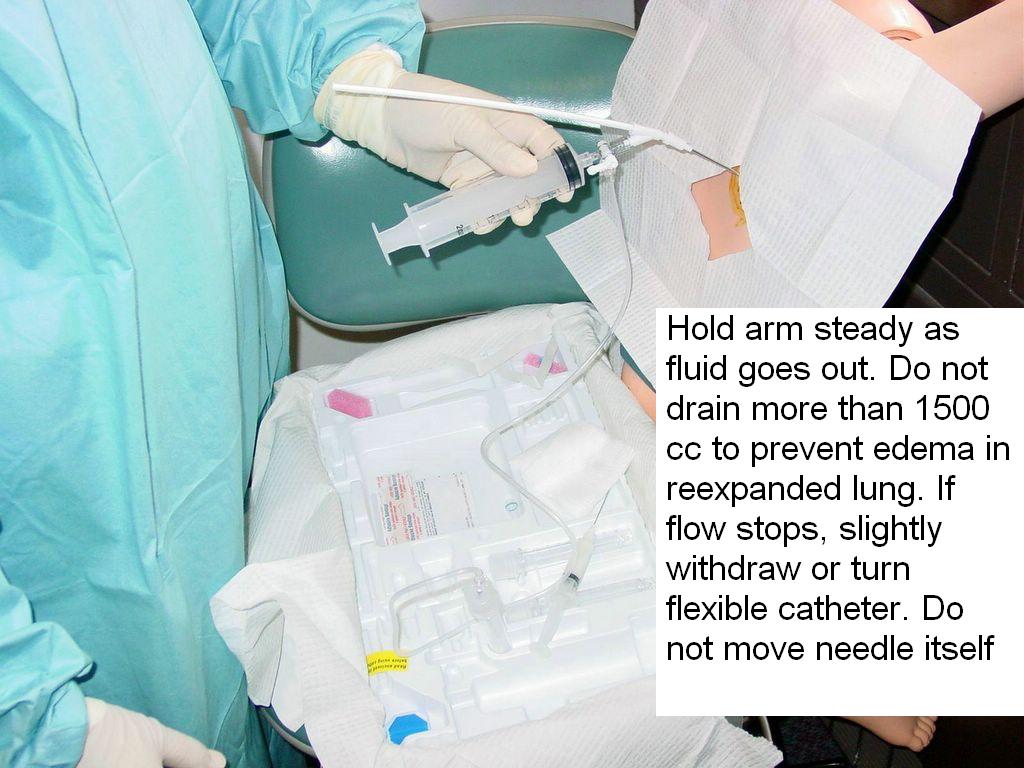
Fig. 21, 22, 23, 24, 25. Pass the flexible catheter over the tap needle into the pleural space and begin aspirating the fluid in the vacuum tubes.

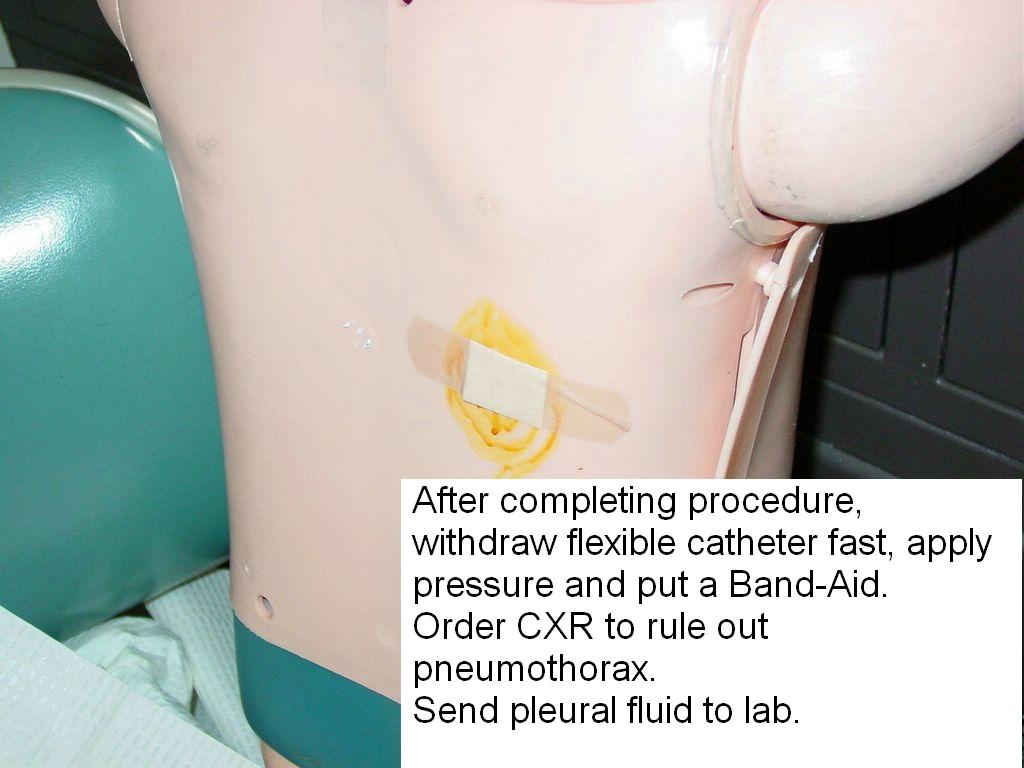
Fig. 26, 27.
Complete the procedure, check for complications - mainly pneumothorax and bleeding. Order a CXR to rule out pneumothorax.
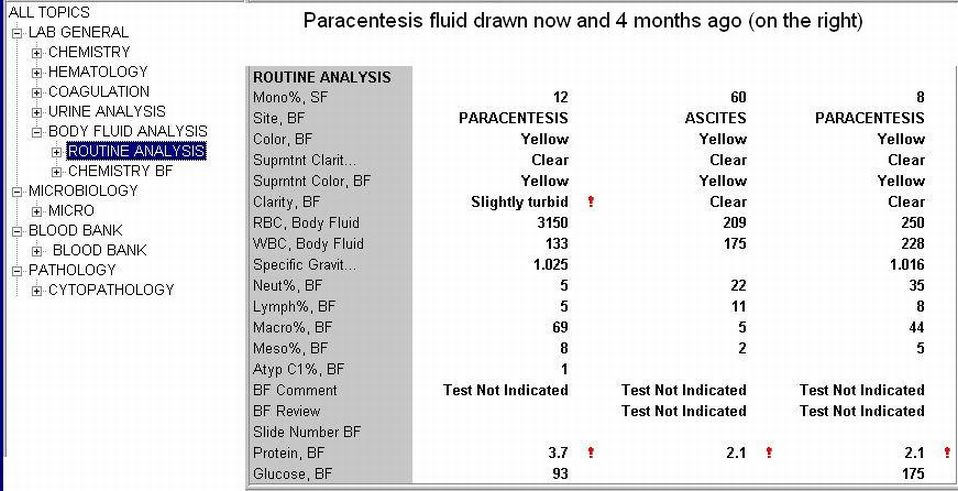
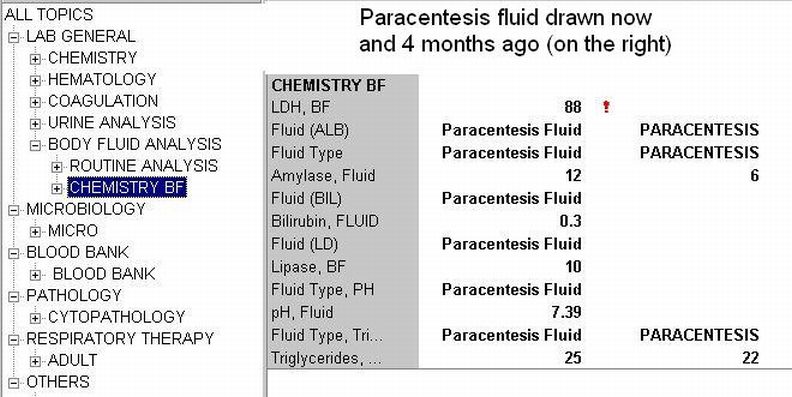
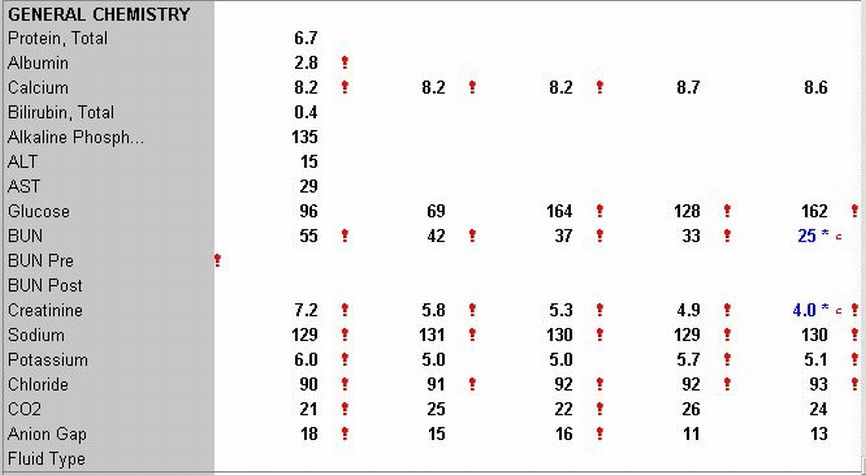
Send the pleural fluid in the 1 L bottle to the laboratory. Compare the pleural fluid to the corresponding blood tests, in order to differentiate between transudate and exudate. If the patient had blood draws this morning, you can order some additional enzymes as AOT (add-on tests), if not already done before the tap.
Complications
Pneumothorax (3-30%)
Hemopneumothorax
Hemorrhage
Hypotension due to a vasovagal response
Pulmonary edema due to lung re expansion
Spleen or liver puncture
Air embolism
Introduction of infection
Write a procedure note which documents the following:
Patient consent
Indications for the procedure
Relevant labs, e.g INR/PTT, platelet count
Procedure technique, sterile prep, anesthetic, amount of fluid obtained, character of fluid, estimated blood loss
Any complications
Tests ordered
References
Thoracentesis. A Chapter in MeisterMed's Procedure Series for PDA. V. Dimov, B. Altaqi, 2/20/2007.
Thoracentesis video from the Loyola University Chicago.
Thoracentesis . The UCSF Hospitalist Handbook.
Thoracentesis video from NEJM, 2006 (paid subscription required).
Diagnostic Approach to Pleural Effusion in Adults. Am Fam Phys, Vol. 73 No. 5, April 1, 2006.
Patient information: Thoracentesis, Medline Plus.
Patient information: Pleural effusion, Medline Plus.
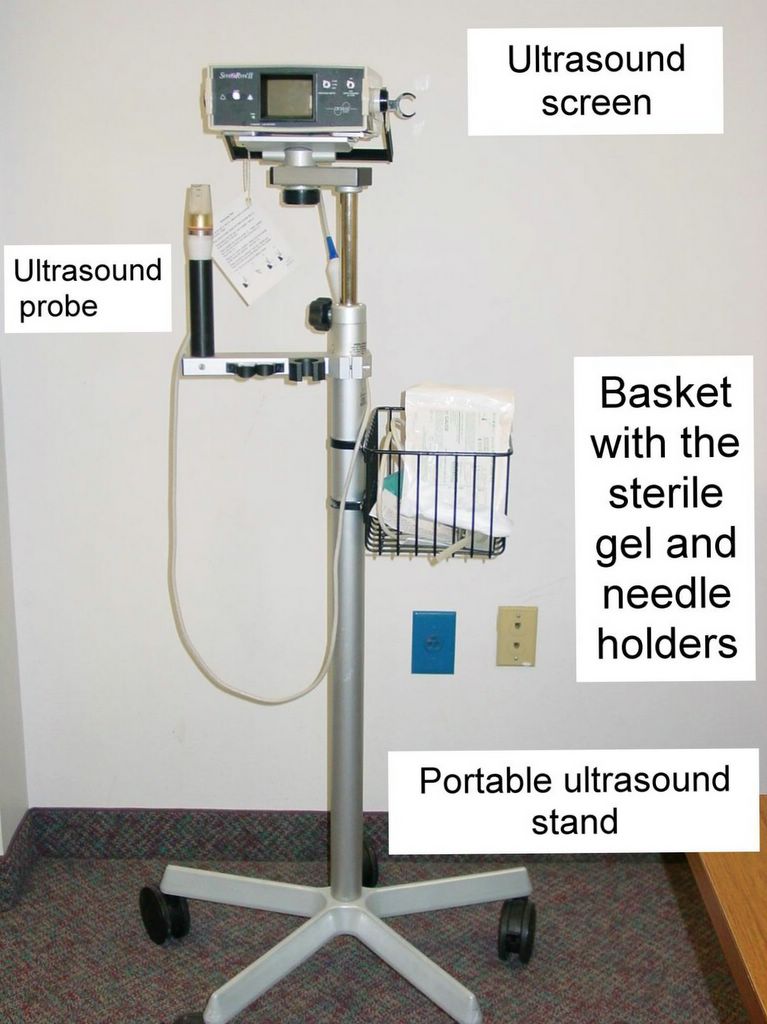
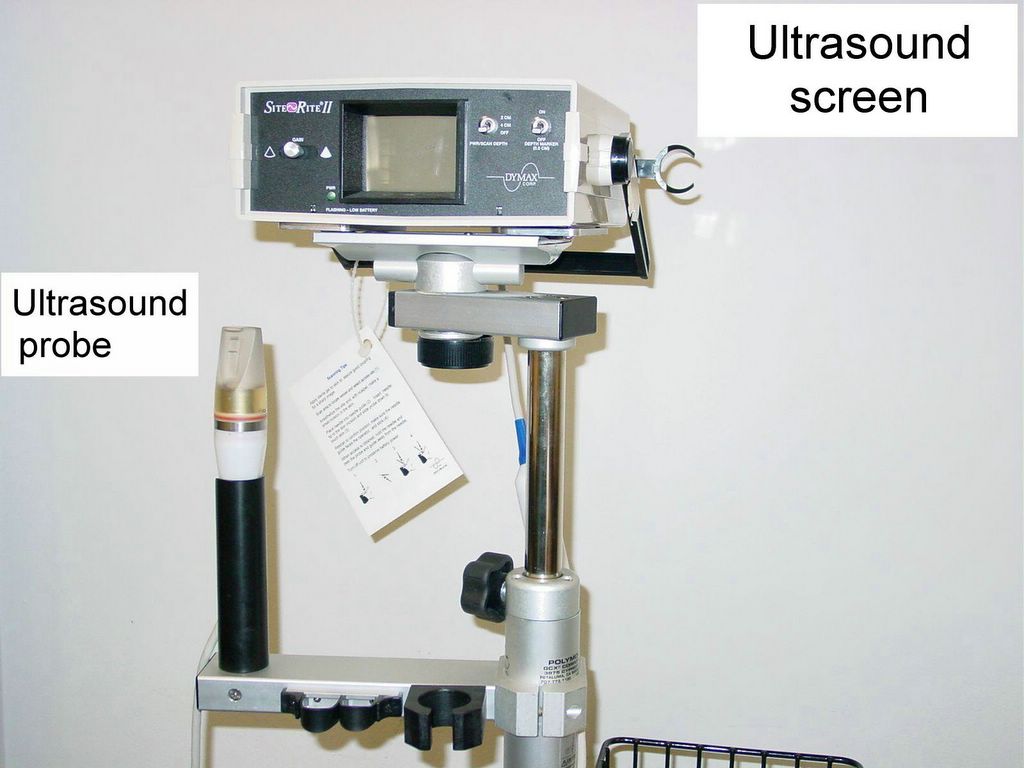
Is Ultrasound-Guided Thoracentesis Safer?, AFP.
Related reading
Becoming a Rural Doctor, Part 5: Procedures for the Rural Doctor. Rural Doctoring, 2008.
Thoracentesis Best Practices: Slideshow. Medscape, 2011.
Disclaimer
The material and/or content on this web site are for informational purposes only. Users of the web site should not act upon any information received from this site without seeking professional consultation. Click here for more information.
Published: 05/11/2005
Updated: 04/17/2008
Disclaimer
The material and/or content on this web site are for informational purposes only. Users of the web site should not act upon any information received from this site without seeking professional consultation. Click here for more information.
Published: 05/11/2005
Updated: 04/17/2008





















{kind=link}